A Real Life Forensic Case Study of GLP-1
Executive Summary: The Setup
At CompoundingAI, we consistently analyze complex systems to identify compounding effects and asymmetrical outcomes. While we typically apply this forensic framework to macro trends such as the pharmaceutical supply chain’s shift toward a chronic annuity model in the metabolic economy**** - occasionally, a micro-level clinical data set emerges that perfectly illustrates how hidden variables dictate massive structural shifts.
This is the forensic tear-down of a recent 30-day metabolic case study involving the 54-year-old mother of one of our team members. On paper, it is a story of a standard Type 2 Diabetes treatment protocol. In reality, it is a masterclass in risk management, the compounding power of concurrent medications, the physics of biomechanics, and the critical importance of de-prescribing.
I. The Baseline and the “Heavy Lifter” Protocol
Diabetes Profile Summary & Trends
| Test Name | Result (21 Mar 26) | Bio. Ref. Interval | Trend: 20 Feb 26 | Trend: 02 Sep 25 | Trend: 06 Jun 25 |
|---|---|---|---|---|---|
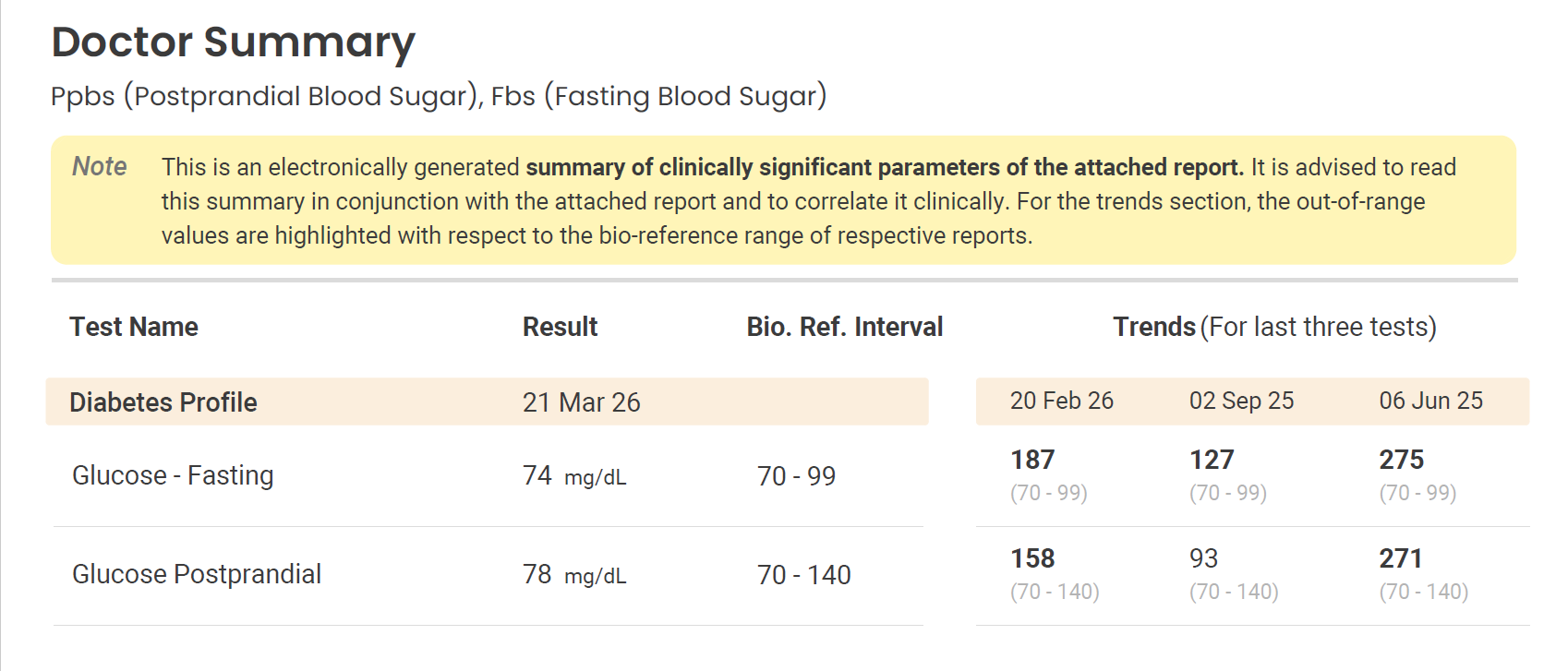
| Glucose - Fasting | 74 mg/dL | 70 - 99 | 187 | 127 | 275 |
| Glucose Postprandial | 78 mg/dL | 70 - 140 | 158 | 93 | 271 |
{kind=link}
Note:* Values in bold* indicate results that were outside the biological reference interval at the time of the test. The most recent results from March 21, 2026, show both fasting and postprandial levels within the normal range.
To understand the magnitude of this anomaly, we must establish the starting metrics. Thirty days prior, the patient presented with a highly elevated Fasting Blood Sugar (FBS) of 187 mg/dL-significantly above the 70-99 mg/dL bio-reference interval.
To aggressively force this number down, the attending physician deployed a heavy, multi-pronged pharmaceutical stack. The oral medications were designed to do the heavy lifting:
- Glykind M 80 MG (Taken 3x/day): A potent blend of Metformin and Gliclazide. Crucially, Gliclazide is a sulfonylurea, it aggressively forces the pancreas to secrete insulin regardless of the patient’s actual blood glucose levels.
- Udapa Trio 500 MG (Taken 1x/day): A triple-combination powerhouse designed to force the kidneys to excrete excess glucose through the urine, alongside additional Metformin.
Into this highly medicated, insulin-heavy environment, the physician introduced a once-weekly GLP-1 receptor agonist (Ozempic 0.25 mg). While we have extensively covered the macro-economics of these therapeutics transitioning into mass-market staples, their micro-physiological effects are equally disruptive. Here, the GLP-1 was deployed to initiate delayed gastric emptying and appetite suppression.
II. The Radical 30-Day Anomaly
Four weeks into the protocol, the patient’s follow-up blood work defied standard linear progression. The results indicated an absolute, radical physiological reset:
- Fasting Blood Sugar: Plummeted from 187 mg/dL to a borderline-low 74 mg/dL.
- Postprandial (PPBS): Following a high-carb stress test (200 ml milk, 30g protein powder, a Vada Pav, and sugarless tea), her blood sugar flatlined at an incredible 78 mg/dL.
- Weight Loss: A massive reduction of 7 kilograms in exactly one month.
- Biomechanical Relief: The spontaneous, complete resolution of chronic knee pain.
- Patient Experience: Reported a surge in energy and highly mindful eating habits, despite a severely suppressed appetite.
Under a standard, flowchart-driven medical protocol, week four dictates a dosage step-up to 0.5 mg of the GLP-1. However, increasing the dose for a patient already sitting at 74 mg/dL while still taking insulin-forcing oral medications introduces a risk of hypoglycemia.
III. The Hidden Variable: The Missing Final Click
During the consultation to address this dilemma, a physical audit of the GLP-1 auto-injector pen revealed a glaring hidden variable: there were still three full doses left in the chamber.
In 30 days, the patient had only received one proper injection. How does a patient mechanically mimic an injection without administering the drug? It comes down to a structural illusion inherent to the device: The Missing Final Click.
When a user presses the top button of the pen, the numerical dial visibly and instantly spins back to zero. Visually, the transaction appears complete. However, GLP-1 medications are highly viscous. The internal spring mechanism requires several extra seconds to physically force the thick liquid through the ultra-fine needle.
The true end of the injection is marked by a final, tactile internal “click” as the spring fully deploys. The patient, seeing the zero, withdrew the needle prematurely. The mechanism halted, trapping the liquid inside and delivering “ghost doses” for three consecutive weeks. This is not an isolated incident; patient troubleshooting data validates the “missing final click” as a real mechanical issue where the dial fails to properly deploy the plunger, leading directly to systemic underdosing.
IV. The Compounding Cascade
This mechanical failure forces a critical question: How did a single 0.25 mg dose drive a 7kg weight loss and a 113-point drop in fasting blood sugar?
The answer lies in metabolic compounding:
- The Long Half-Life: Semaglutide has a highly resilient half-life. That single, successful Day 1 dose remained active in her system for weeks, successfully triggering the satiety signals in the brain and slowing digestion.
- The Oral Engine: While the GLP-1 suppressed her urge to eat, the heavy oral stack (specifically the 3x/day Gliclazide) continued to relentlessly force her pancreas to pump out insulin.
- The Extreme Caloric Deficit: With an artificially high insulin presence, continuous glucose excretion from the kidneys, and a sudden, massive drop in caloric intake, the body was forced into an aggressive state of rapid fat oxidation.
The single GLP-1 dose compounded with the aggressive baseline prescription to create an outsized, asymmetrical physiological response. Furthermore, emerging empirical data supports this biological resilience. A March 2026 study found that patients could maintain significant weight loss by reducing injection frequency to once every two to six weeks, validating the “One-Dose Anomaly” as a potential clinical reality and pointing toward a broader, structural trend of dose-sparing.
V. The Secondary Derivative: Biomechanical Compounding
In complex systems, a primary catalyst often triggers massive secondary derivatives. While the metabolic reset was the primary headline, the 7-kilogram weight loss initiated a profound structural compounding effect: the resolution of the patient’s chronic knee pain.
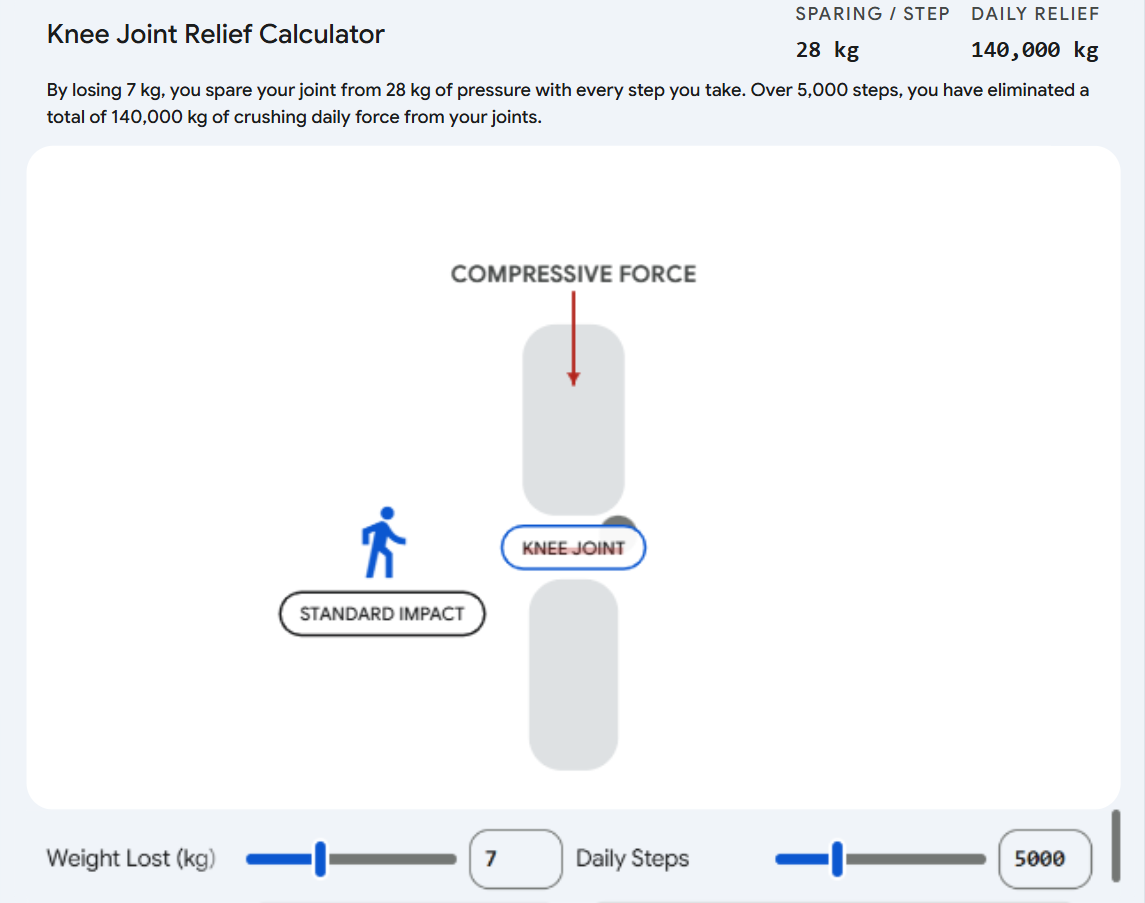
In the physics of human locomotion, this is governed by the “4-to-1 Rule.” During level walking, the compressive force exerted on the knee joint is roughly four times total body weight. Therefore, for every 1 kilogram of mass lost, 4 kilograms of destructive load are removed from the joint per step.
By shedding 7 kg, the patient effectively removed 28 kg of compressive force every time her foot struck the ground. Assuming a conservative baseline of 5,000 daily steps, this equates to 140,000 kg of cumulative mechanical stress eliminated from her joints every single day.
{kind=link}
This structural relief allowed for the immediate de-prescribing of her legacy pain and anti-inflammatory medications (ASEC SP), further reducing her overall pharmaceutical load.
VI. The Pivot: Risk Management and De-prescribing
Faced with this data, the physician executed a masterclass in clinical risk management.
If the patient achieved 74 mg/dL with effectively zero continuous GLP-1 support, actually adhering to a weekly 0.25 mg schedule going forward would overwhelm her system. Instead of escalating the GLP-1 to 0.5 mg, the doctor pivoted to de-prescribing.
He immediately cut the aggressive oral medications with Gliclazide and Metformin by half, removing the artificial floor under her blood sugar to prevent a hypoglycemic crash. Simultaneously, he locked the GLP-1 dosage at the introductory 0.25 mg, ensuring proper mechanical administration moving forward.
Core Read-Through
Whether analyzing a corporate balance sheet or a patient’s metabolic profile, the lesson remains constant: outsized outcomes are rarely the result of linear progression. They are driven by compounding variables interacting within a system. By identifying the mechanical anomaly (the missing click) and intelligently de-prescribing the legacy oral stack, the physician successfully optimized the patient’s baseline without risking systemic failure.
Thanks for reading. This post is public so feel free to share it.
Note : This only for educational purpose. Not a medical advice or recommendation.
CompoundingAI is a vertical intelligence engine that transforms unstructured documents into decision-grade insights, complete with source-level traceability for confident, auditable workflows.
We cut the noise & directly deliver insights.
Powered by CompoundingAI — AI research platform for Indian stocks, every claim cited from primary filings
Login Now